

The burden of HAE
HAE places a substantial burden on patient Quality of Life (QoL)
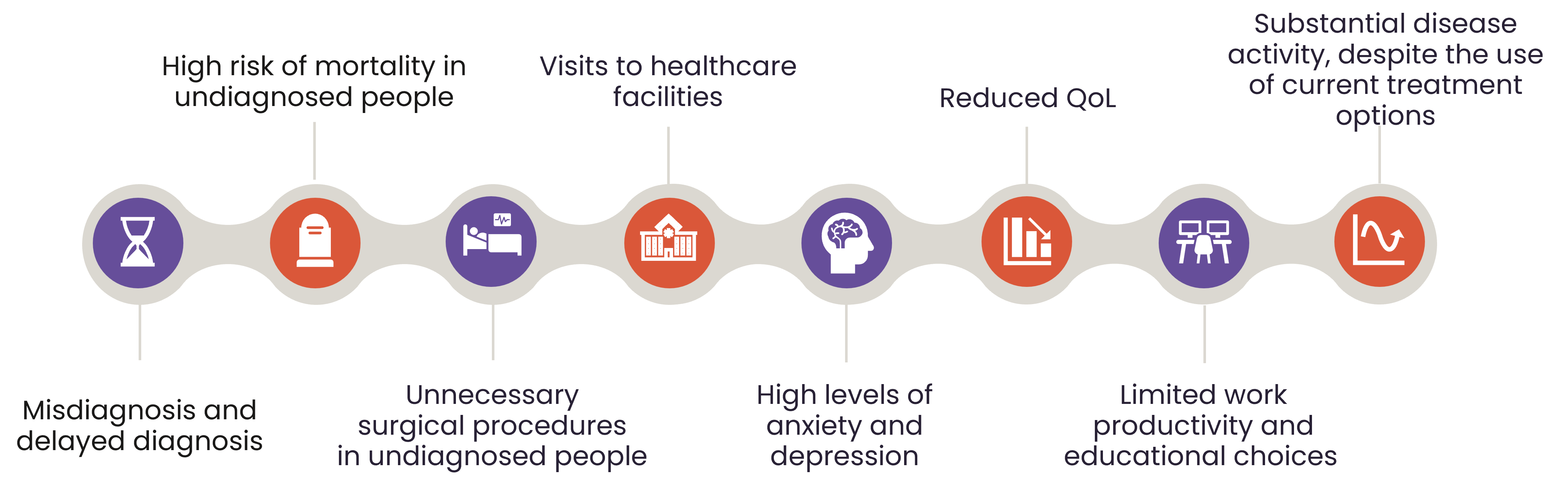
HAE imposes a substantial burden on patients, through its impact on physical, psychological/emotional, and social factors.1
The unpredictability of HAE means that patients are impacted not only during attacks, but also between attacks.2

Impact during attacks
In one study, 87% of patients described HAE-related abdominal pain as “severe to excruciating”, with some saying that they could not imagine more severe pain.5
In a multinational survey, patients with HAE reported:4
- Absence from work for 8% of the prior week
- A 24% loss in work productivity
Impact between attacks
In a multinational survey of 242 patients with HAE:4
- 44.3% of patients report being ‘much’ or ‘very much’ bothered by the unpredictability of HAE attacks
- 38.0% of patients report moderate to severe anxiety
- 17.4% of patients report moderate to severe depression
Due to the genetic nature of HAE, patients may have ancestors who have died due to asphyxiation, which could worsen their worries about attacks.1 One study found that almost three quarters of patients with HAE worried about asphyxiating, greatly impacting their psychological wellbeing. This percentage was reduced to 38% after patients were taught to self-administer medication.8
The Burden of HAE
Bork K, et al. 2012;3 Mendivil J, et al. 2021;4 Banerji A, et al. 2020;9 Lumry W, Settipane R. 20207
Unmet need in HAE treatment
In a 2019 multinational survey of patients with HAE, despite 62% of patients receiving LTP, patients reported a mean of 12.5 attacks in the past 6 months.4

As long as patients continue to experience attacks, there is still a need to develop new, more effective and more convenient treatments.

What is HAE?
Learn about HAE, including mechanism of disease, symptoms, triggers and diagnosis

Goals of HAE treatment and available treatment options
Find out the goals of HAE treatment and treatment recommendations
Considerations for special patient populations
Learn how to manage HAE in special populations
References
- Bygum A, Busse P, Caballero T, Maurer M. Disease Severity, Activity, Impact, and Control and How to Assess Them in Patients with Hereditary Angioedema. Front Med (Lausanne). 2017;4:212.
- Bork K, Anderson JT, Caballero T, Craig T, Johnston DT, Li HH, et al. Assessment and management of disease burden and quality of life in patients with hereditary angioedema: a consensus report. Allergy Asthma Clin Immunol. 2021;17(1):40.
- Bork K, Hardt J, Witzke G. Fatal laryngeal attacks and mortality in hereditary angioedema due to C1-INH deficiency. J Allergy Clin Immunol. 2012;130(3):692-7.
- Mendivil J, Murphy R, de la Cruz M, Janssen E, Boysen HB, Jain G, et al. Clinical characteristics and burden of illness in patients with hereditary angioedema: findings from a multinational patient survey. Orphanet J Rare Dis. 2021;16(1):94.
- Bork K, Staubach P, Eckardt AJ, Hardt J. Symptoms, Course, and Complications of Abdominal Attacks in Hereditary Angioedema Due to C1 Inhibitor Deficiency. Am J Gastroenterol. 2006;101(3):619-27.
- Aygören-Pürsün E, Bygum A, Beusterien K, Hautamaki E, Sisic Z, Wait S, et al. Socioeconomic burden of hereditary angioedema: results from the hereditary angioedema burden of illness study in Europe. Orphanet J Rare Dis. 2014;9:99.
- Lumry WR, Settipane RA. Hereditary angioedema: Epidemiology and burden of disease. Allergy Asthma Proc. 2020;41(Suppl 1):S08-s13.
- Bygum A. Hereditary angioedema - consequences of a new treatment paradigm in Denmark. Acta Derm Venereol. 2014;94(4):436-41.
- Banerji A, Davis KH, Brown TM, Hollis K, Hunter SM, Long J, et al. Patient-reported burden of hereditary angioedema: findings from a patient survey in the United States. Ann Allergy Asthma Immunol. 2020;124(6):600-7.
- Longhurst HJ, Bork K. Hereditary angioedema: an update on causes, manifestations and treatment. Br J Hosp Med (Lond). 2019;80(7):391-8.
- Craig TJ, Banerji A, Riedl MA, Best JM, Rosselli J, Hahn R, et al. Caregivers' role in managing hereditary angioedema and perceptions of treatment-related burden. Allergy Asthma Proc. 2021;42(3):S11-s6.
DNK-AND-0001, 25/04/25